

The Norwood Pathway:
Standardizing Care to Improve Outcomes
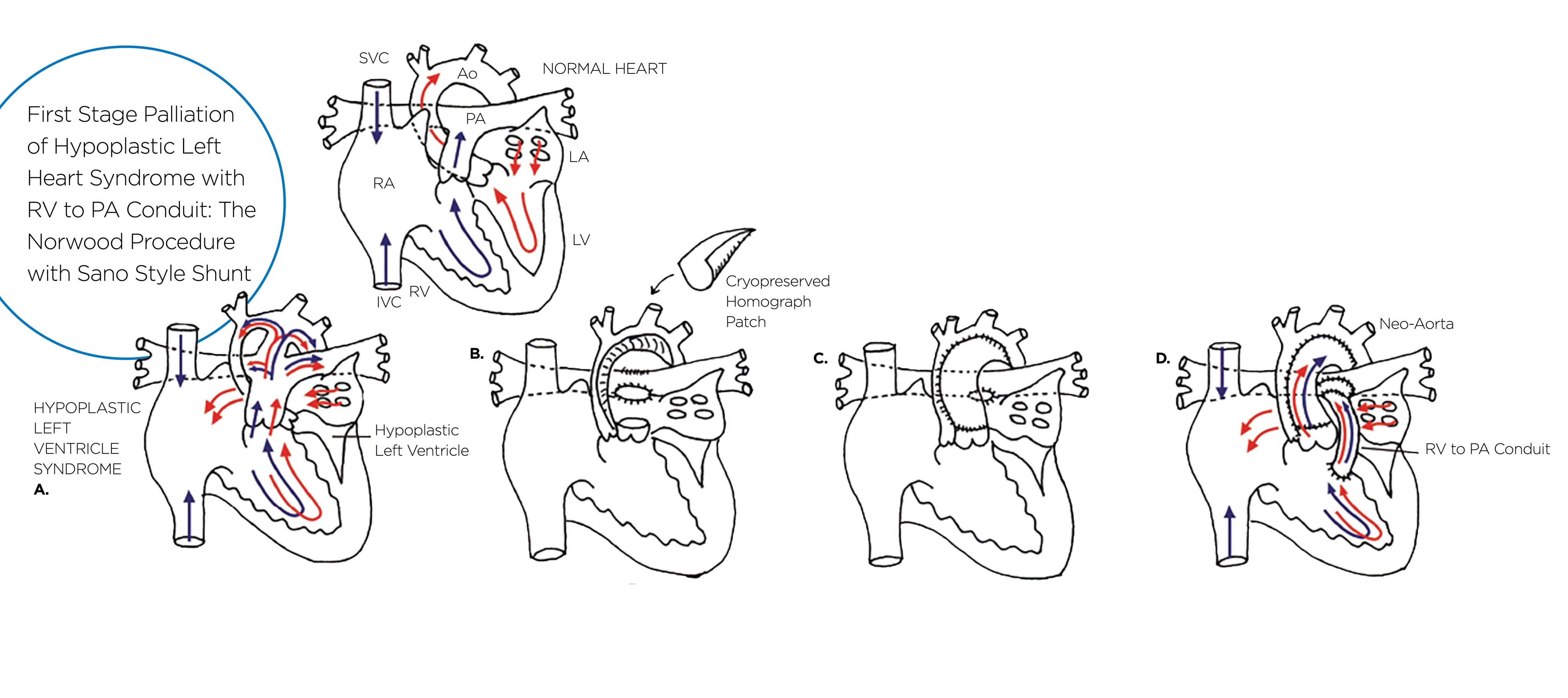
At Children’s Wisconsin, we know the Norwood operation remains one of the most complex and high-risk congenital heart surgeries. This procedure is typically performed in the first week of life for infants born with hypoplastic left heart syndrome (HLHS). It is the first of three staged surgeries designed to enable the right ventricle to pump blood to the body and establish pulmonary blood flow.¹ Our team at the Herma Heart Institute has long been recognized as a leader in advancing outcomes for these critically ill children.² ³ Still, we recently experienced a decline in survival rates, which led us to take a closer look at the procedure.
In 2023, we formed a multidisciplinary group to develop a structured pathway for the Norwood operation. Our goal was to standardize communication and care through all stages of perioperative management. The team included clinicians from pediatric cardiovascular surgery, cardiology, cardiac anesthesia, cardiac intensive care, perfusion and nursing. Over a series of collaborative meetings, we created algorithms and guidelines that became the Norwood Pathway. These were based on both published data and accepted standards of care across top pediatric surgical centers. Once it was finalized, we shared the pathway broadly throughout the Herma Heart Institute.
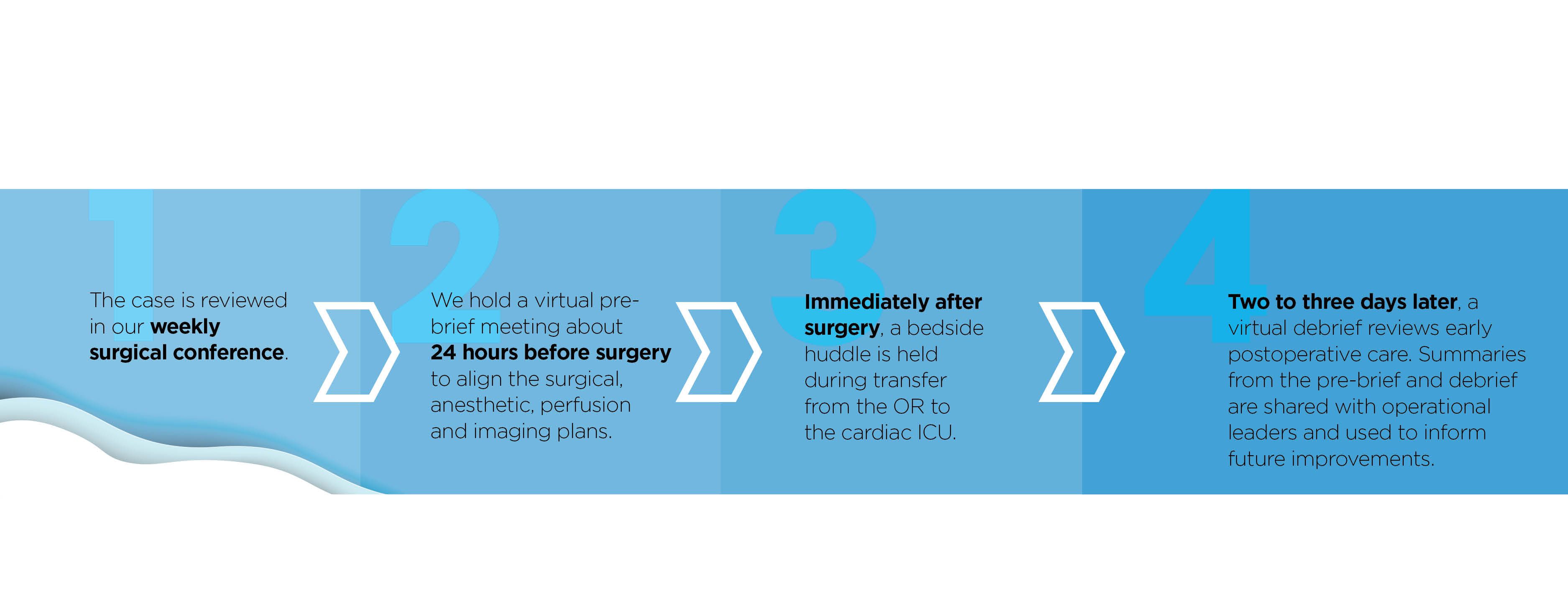
One of our primary aims was to improve communication. For every patient undergoing a Norwood procedure, we now conduct four standardized discussions:
1. The case is reviewed in our weekly surgical conference.
2. We hold a virtual pre-brief meeting about 24 hours before surgery to align the surgical, anesthetic, perfusion and imaging plans.
3. Immediately after surgery, a bedside huddle is held during transfer from the OR to the cardiac ICU.
4. Two to three days later, a virtual debrief reviews early postoperative care. Summaries from the pre-brief and debrief are shared with operational leaders and used to inform future improvements.
These regular touchpoints have allowed us to make data-informed changes to the pathway. In the past two years, we have adjusted aspects such as shunt characteristics, surgical techniques and inotrope management based on real-time learning.


Since implementing the pathway, we have cared for 20 Norwood patients using this model. Survival has improved from 69% to 85%. Median cardiac ICU length of stay is now 20.5 days, slightly below the national average of 21.1 days and a 50% reduction compared to our pre-pathway data. Median hospital stay is now 39 days compared to our prior local average of 80 days and the national benchmark of 36 days. We have also maintained low rates of deviation from the pathway, with 7% overall variation and just 2% classified as unintentional.
As we look to the future, we will continue to refine our approach and measure results. We plan to share the Norwood Pathway with our partners at UW Health Kids and American Family Children’s Hospital through the Forward Pediatric Alliance. Our goal is not only to improve survival but to reduce the burden of morbidity and support the best possible outcomes for every child undergoing this complex surgery.
By aligning our teams and standardizing our practices, we are building a care model that is not only collaborative but also adaptable. We are proud of the progress we have made and are committed to continuing this work to improve the lives of children with HLHS and their families.
References
1. John MM, McKenzie ED. Norwood procedure: How I do it. JTCVS Techniques. 2020 December;4:P205-7.
2. Tweddell JS, Hoffman GM, Mussatto KA, Fedderly RT, Berger S, Jaquiss RD, Ghanayem NS, Frisbee SJ, Litwin SB. Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: lessons learned from 115 consecutive patients. Circulation. 2002 Sept;106.I82-9.
3. Hoffman GM, Ghanayem NS, Scott JP, Tweddell JS, Mitchell ME, Mussatto KA. Postoperative cerebral and somatic near-infrared spectroscopy saturations and outcomes in hypoplastic left heart syndrome. Ann Thorac Surg. 2017 May;103:1527-35.