
Multiple Procedures Under One Anesthetic: Guidance for Care
When families are told their child needs surgery or a procedure under anesthesia, one of the first questions they ask is: “Is it safe?” That concern often deepens when multiple procedures are under consideration. Understandably, many families ask us if combining procedures in one visit is a safer, more efficient option.
As pediatric anesthesiologists at Children’s Wisconsin, we’ve explored that question through experience and data. With the increasing demand for coordinated care, we wanted to understand whether combining procedures increases risk or can be done safely under the right conditions.
Pediatric procedures carry risk from both anesthesia and the underlying surgery. These risks depend on patient complexity, age, procedure duration and other variables. Risks can become more complex when unrelated procedures, managed by different specialties, are scheduled together.
To explore this, we began analyzing perioperative outcomes in line with our participation in the American College of Surgeons Level I Children’s Surgery Verification Improvement Program.
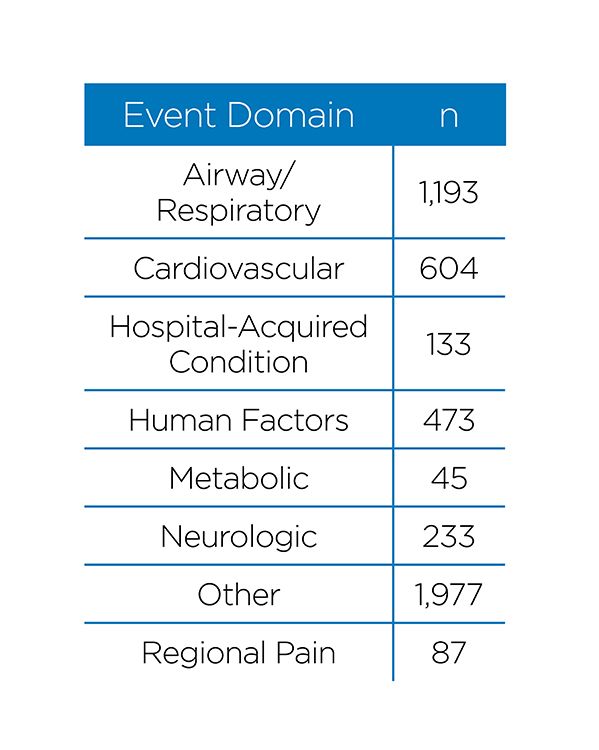
Since June 2015, our department has recorded more than 219,000 anesthetic cases involving nearly 120,000 children. We identified 2,490 perioperative events, categorized into eight domains: airway/respiratory, cardiovascular, hospital-acquired conditions, human factors, metabolic, neurologic, regional pain and an “other” category for access issues, drug effects, allergic reactions and unexpected returns to care areas.

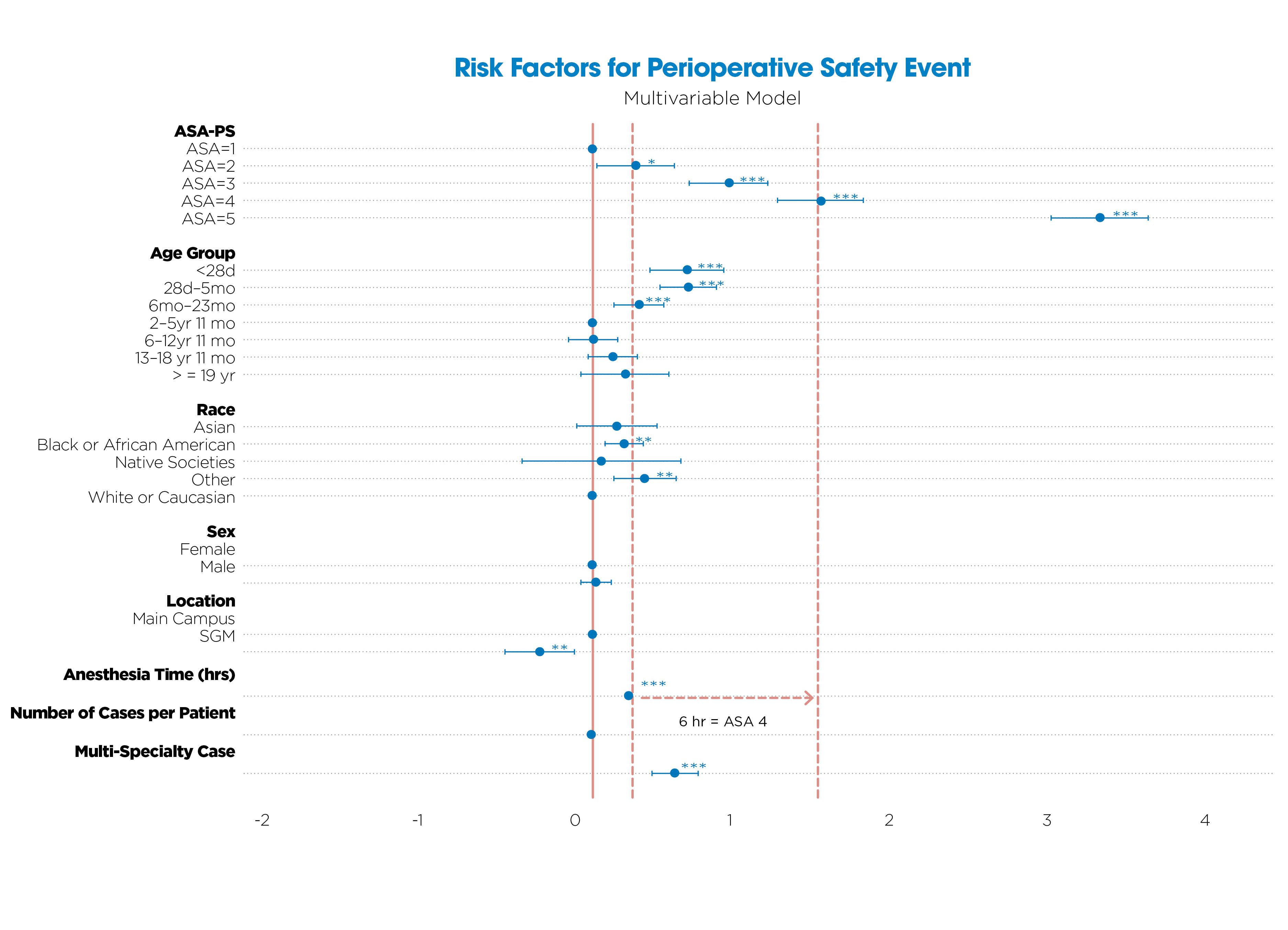
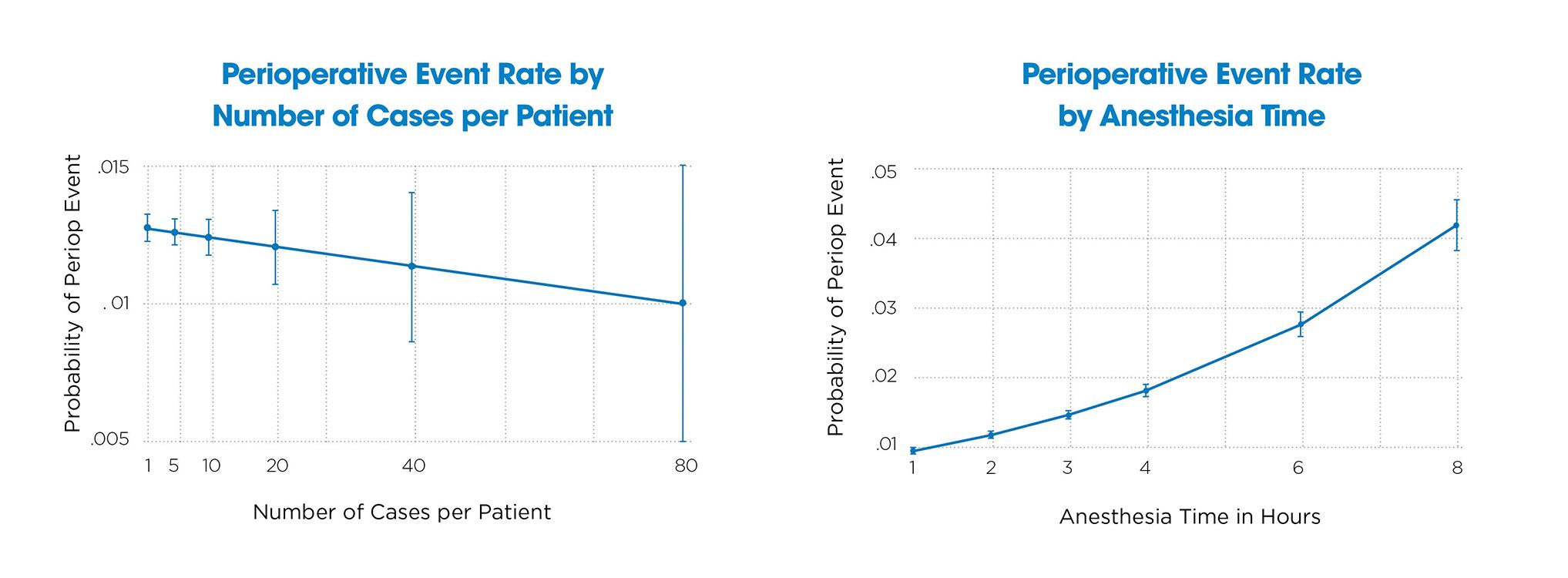
We examined these outcomes against factors such as ASA physical status, age, race, anesthesia time and whether the care involved a single specialty or multiple, unrelated specialties (multi-specialty). Our multivariable analysis confirmed that higher ASA scores, younger age, Black race, longer anesthesia times and multi-specialty care were all independent predictors of perioperative events. For example, six hours of anesthesia carried a risk comparable to ASA-PS 4. Importantly, we found that multiple separate anesthetics did not increase risk, but prolonged time under a single anesthetic did.
We also recognized that not all complications carry equal weight. A mild IV infiltration isn’t equivalent to a serious cardiac event. To address this, we implemented a standardized scoring system to assess the severity of each event: none, mild, moderate, severe or death. This allows us to distinguish between minor issues and serious complications and supports more precise decision-making.
To improve detection and reporting, we now use our electronic health record (EHR) to monitor and flag perioperative events. While intraoperative complications are often recorded in real time, others may occur postoperatively or be missed if not proactively identified. Our EHR-based surveillance allows us to detect these events independently of clinician self-reporting, ensuring a complete and more reliable dataset.
We’re not alone in asking whether combining procedures poses additional risk. Literature from other institutions reinforces what we’re finding. One study found time and cost benefits in children who had dental restorations and extractions done under a single anesthetic, with no reported increase in complications.¹ Another group examined combined dental and tonsillectomy procedures and found no difference in outcomes compared to when performed separately.² Lastly, a large study covering more than 1,100 cases found no increase in readmissions for multi-specialty procedures.³


Of course, any plan of care must also consider the broader family experience. Scheduling multiple procedures separately can mean more days off work, missed school and stress. Reducing the number of anesthetic exposures and consolidating care, when safe and feasible, can ease the burden on families and the system alike.
Ultimately, our goal is to provide data-informed guidance. With more than 200,000 cases analyzed, we now have a clearer view of what increases risk and what doesn’t. We can better advise families, offer safer care and align our decisions with evidence and empathy.
We know that every child and every family situation is different. But with the right planning, communication and monitoring, we’ve shown that many children can safely undergo more than one procedure under a single anesthetic. The key is understanding and acting on the true risk with clarity, precision and compassion.

References
1. Stapleton M, et al. One visit or two? Time and cost benefits of combining dental procedures under one anesthetic. J Clin Pediatr Dent. 2007.
2. Syed F, et al. Perioperative outcomes of combined dental and tonsillectomy procedures in pediatric patients. Int J Pediatr Otorhinolaryngol. 2018.
3. Miketic M, et al. Safety of combining unrelated surgical procedures under a single anesthetic. J Pediatr Surg. 2019.